New health challenges call for a new approach
The emergency phase of the pandemic is drawing to a close, but the NHS has a daunting to-do list stretching well into the future. Overhauling an under-appreciated component of the health service, the payment system, can help it rise to its evolving challenges.
Payments systems matter. It is partly through the payment system that the NHS allocates resources to providers and providers decide on their priorities. That has long been recognised as payment reforms have reflected shifting objectives for the NHS.
Before the pandemic, the NHS was already considering replacing the activity based system for hospital payment (payment by results (PBR)) with a ‘blended’ approach to payment. We believe that this is the right approach and that the blended payment should have three core components
- A fixed payment element to secure adequate supply of health care services. This would be set to cover the operational costs of providing the level of acute services agreed within population-level planning agreements.
- A variable component to adjust payments to reflect differences between planned and actual levels of activity.
- A quality component to incentivise and fund quality of care in priority areas.
If designed well, a three-part payment system could help ensure the NHS has the right capacity in the right place. By making it easier to juggle resources, the flexibility of the set-up would help the NHS whittle down a long backlog of elective caseloads and achieve its ambitious longer-term goals. These include a shift of more services out of hospitals and into community and primary care settings, better health management of an ageing population and the reduction.
Figure 1: Framework for the hospital, community and mental health payment system
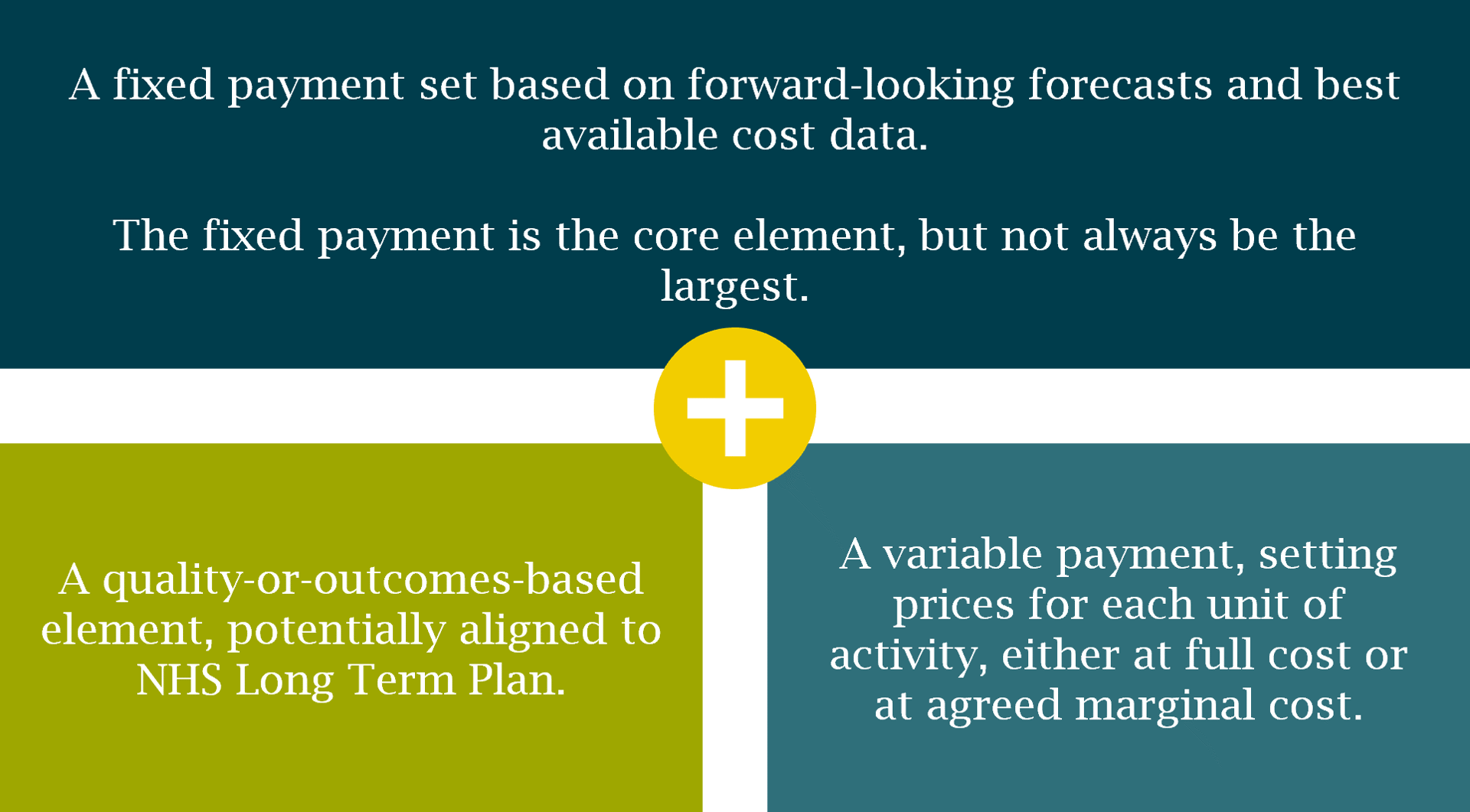
Source: Previously published NHS England consultation paper.
Three big issues for a blended payment system to address
Although a blended payment system is the right direction of travel, detailed design work in the coming months needs to address some important issues.
The NHS therefore needs to build in greater resilience and flexibility . That means the payment system has to weigh the risk of failure due to insufficient standby capacity against the cost of strengthening the system’s resilience to external shocks by paying for beds and equipment that may well gather dust.
A second key question is how to provide the right incentives to providers to meet the challenge of the elective care backlog. More than 300,000 people have been waiting more than a year for planned care, compared with around 1,500 in December 2019. As of April 2021, the total waiting list numbered 4.7m, and modelling work projects that without a significant increase in activity, that number could double by 2023/24. Activity based payments could support providers efforts to tackle the backlog.
Activity based payments must be attractive enough to encourage providers to flex their capacity and deliver more care, but without diverting too much attention and resource to the detriment of other services. It will also be important to work out a fair tariff for independent sector providers if they are to offer additional capacity – properly understanding private sector costs must sit alongside the NHS cost structures and, if they differ, developing tariffs that reflect legitimate differences.
A third fundamental decision will be to ensure that quality payments are sufficient to incentivise high quality services as well as high volume services. While quality in the NHS is encouraged and ensured by factors that go far beyond payment systems, it is nonetheless important that where financial incentives are deployed they are of a sufficient size and well enough targeted to get the desired result. There is a wide international evidence base to draw upon as these are designed as well as experience in England relating to CQUINs (which may be too small in scale to have much impact) and the GP Quality and Outcomes Framework.
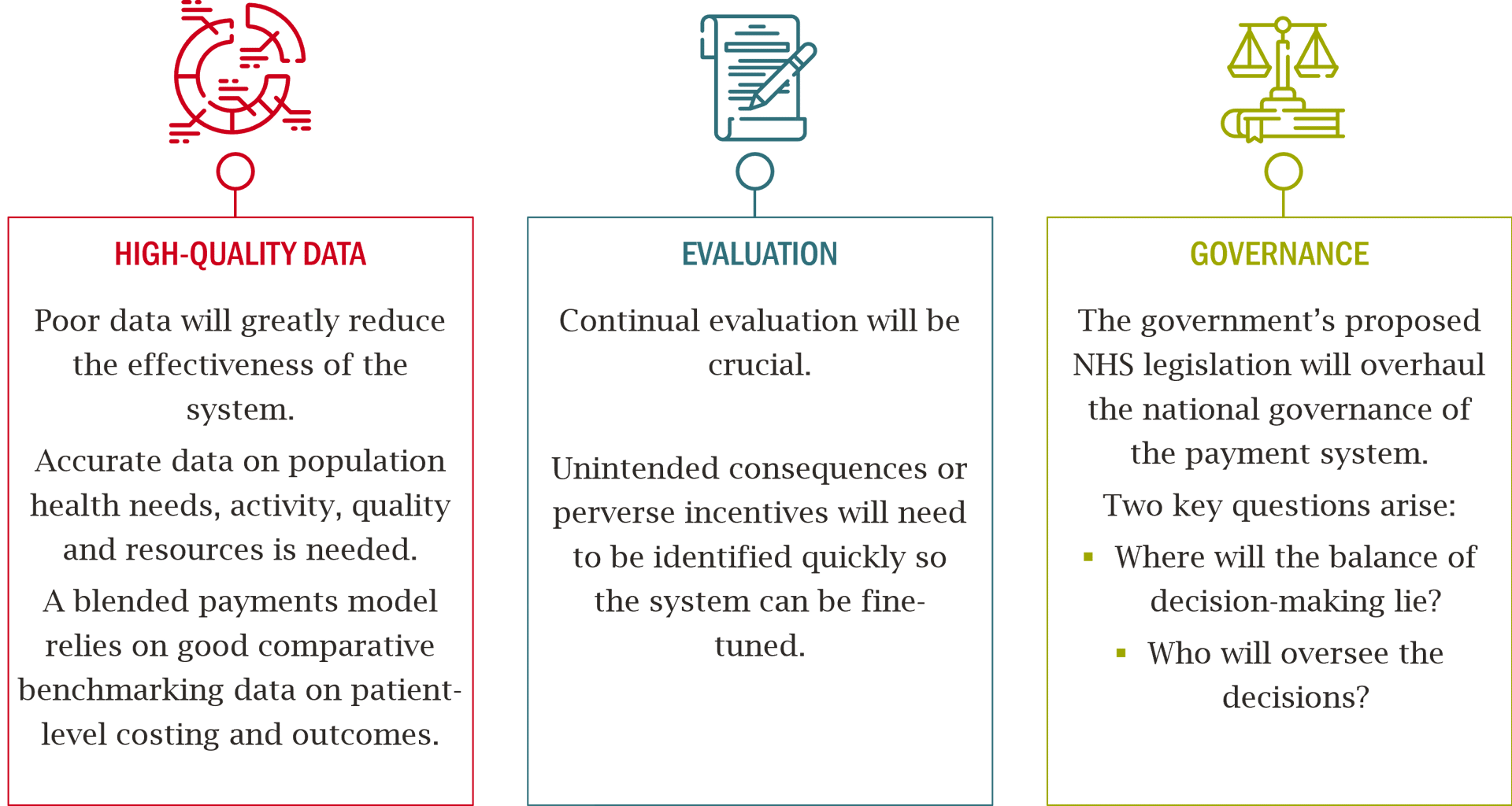
Three essential features of a blended payment system
Beyond the design of fixed, activity and quality payments, an effective post-pandemic payment system needs to incorporate a number of other essential features. These include:
Conclusion
The UK is entering the post-COVID recovery phase. As part of that process, a transformation of the NHS is required to meet a different, but no less daunting, set of challenges. A new payment system can play a part in supporting such a transformation.
A sustainable health system needs to use public funds efficiently, to adapt to changing patient needs and to respond to public expectations. Critically, incentives in the payment system must be designed to encourage all parties to work towards the same goals. Replacing an approach dominated by one set of payment incentives (PbR) (albeit with other elements) with something more explicitly nuanced feels like the right response.
The good news for the NHS is that there appears to be a growing consensus that a new approach is required. The challenge will be addressing the complexities that sit behind the headlines, some of which we have outlined here.
Co-authored by Richard Lewis, Associate in the Public Policy practice and Anita Charlesworth, Director of Research and the REAL Centre at the Health Foundation.
This article is based on the Health Foundation’s briefing paper, The future of the NHS hospital payment system in England and the Health Service Journal’s commentary, How the new payment system for the NHS could succeed or fail.